Head and neck cancer
Head and neck cancer arises in the nasal cavity, sinuses, lips, mouth, salivary glands, throat, or larynx (voice box). Head and neck cancers are common in several regions of the world where tobacco usage and alcohol consumption is high. The age standardized incidence rate in males exceeds 30/100,000 in regions of France, Hong Kong, the Indian subcontinent, Central and Eastern Europe, Spain, Italy, Brazil, and among US African Americans. High rates (>10/100,000) in females are found in the Indian subcontinent, Hong Kong and Philippines. Of all newly diagnosed cancers, head and neck cancers comprise approximately 10% in the western world, but one third in India. The variation in incidence by sub-site of head and neck is mostly related to the relative distribution of major risk factors such as tobacco or betel quid chewing, cigarette or bidi smoking, and alcohol consumption.
There is increasing evidence that viruses contribute to the cause of head and neck cancer. DNA from human papilloma virus (HPV) has been detected in cancerous tissue from head and neck and infection with Epstein-Barr virus is associated with nasopharyngeal cancer. Surprisingly, patients with advanced forms of cancer in the upper portion of the throat have better outcome if the tumor is positive for HPV. Occurrence of head and neck cancer in young adults and in non-users of tobacco and alcohol suggests that genetic predisposition may be a possible etiologic factor.
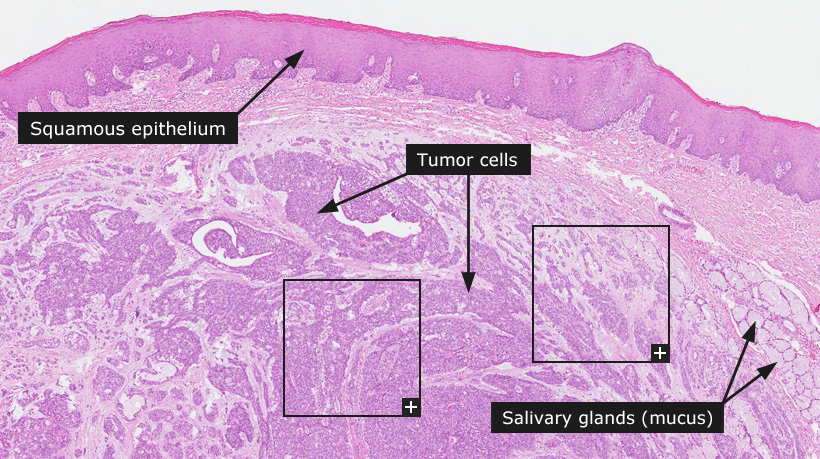
Most head and neck cancers arise from squamous epithelium and are squamous cell carcinomas of different histologic grades. The tumor cells in well-differentiated cancers closely resemble normal squamous epithelium, whereas poorly differentiated cancers are difficult to classify as being of squamous epithelial origin. Salivary gland tumors (mainly adenocarcinomas) comprise a minority of head and neck tumors. Squamous and salivary gland carcinomas spread by direct contiguity and by the lymphatic route draining into the regional lymph nodes.
The most widely used system for staging cancer is called the TNM System. It describes the extent of the primary tumor (T stage), the absence or presence of spread to nearby lymph nodes (N stage) and the absence or presence of distant spread, or metastasis (M stage). Once the T, N and M are determined, a stage of I, II, III or IV is assigned. Stage I cancers are small, localized and usually curable, while stage II and III cancers typically are locally advanced and/or have spread to local lymph nodes. Stage IV cancers are usually metastatic (have spread to distant parts of the body) and are generally considered inoperable. Early stage (Stage I and II) cancers yield a 60-95% cure rate that falls to 25% for Stage IV tumors.
Normal tissue: Salivary gland, Oral mucosa
 The Human Protein Atlas project is funded
The Human Protein Atlas project is funded



 MENU
MENU