The cancer proteome
A large number of genes with diverse normal functions are involved in human cancer. More than 500 genes have been identified as strongly implicated in the process of transforming normal cells to cancer cells. The expression of these genes in normal cells contributes to normal growth, survival and function, whereas dysregulated expression, including overexpression, loss of expression or expression of a defect protein, in cancer cells contributes to ungoverned tumor growth. Altered gene expression can be caused by coarse structural and numerical chromosomal rearrangements, specific gene amplifications, silencing of transcription through methylation and mutations, e.g. point mutations with single base substitutions and small inserts or deletions, that lead to loss or gain of function of the corresponding protein.
Genes and Proteins Altered in Cancer
Currently, more than 1% of all human genes are implicated via mutation in cancer. Of these, approximately 90% have somatic mutations in cancer, 20% bear germline mutations that predispose to cancer and 10% show both somatic and germline mutations. A list of genes strongly implicated in cancer (n=599) has been defined through the cancer Gene Census, catalogue of somatic mutations in cancer (COSMIC).
Table 1. List of different genetic alterations in 599 genes that are implicated in cancer.
| Genetic alteration |
Number of genes |
| Somatic Mutations |
558 |
| Translocations |
345 |
| Missense Mutations |
242 |
| Nonsense Mutations |
152 |
| Frameshift Mutations |
150 |
| Germline Mutations |
100 |
| Splicing Mutations |
75 |
| Large Deletions |
40 |
| Other Mutations |
37 |
| Amplifications |
18 |
| Total number of mutated genes |
599 |
It is clear that we are far from having a complete catalogue of cancer genes and results from efforts to identify genetic alterations implicated in cancer are continuously being published. In a recent study from the Broad Institute (Lawrence MS et al., 2014), a list of 260 significantly mutated cancer genes across 21 cancer types is presented, of which 259 are present in the current version of the Human Protein Atlas. In another study aiming to identify cancer driver genes (Tamborero D et al., 2013), a list of 291 high-confidence cancer driver genes across 12 cancer types is presented, of which 285 are present in the current version of the Human Protein Atlas.
Protein expression of cancer genes
Protein profiling using immunohistochemistry allows for visualization of the distribution and relative abundance of proteins encoded by cancer genes in various tumor tissues. Certain proteins show differential expression between different forms of cancer or individual tumors within the same form of cancer whereas other proteins show variable expression within different compartments of the tumor or in tumor cells of different states. Moreover, differences in expression can be found between tumors and corresponding normal tissue counterparts. Below are a few examples of protein expression patterns in different forms of cancer and normal tissues.
Figure 1. Immunohistochemical staining patterns in normal and cancer tissue corresponding to a few examples of genes implicated in cancer.
Cancer
Cancer can be defined as a common heterogeneous and potentially deadly disease that affects approximately a third of the human population. The common denominator for cancer
is the development of an uncontrolled growth of cells that eventually leads to multiple organ failure and death. Cancer can be classified into several different diseases depending on
the organ where the primary cancer develops and on the type of cancer (microscopical and molecular features of the tumor). Lung cancer,
breast cancer, colorectal cancer,
stomach cancer, liver cancer and
cervical cancer are the most common forms of cancer worldwide. Epidemiologic research can provide
cancer statistics regarding the incidence, prevalence and mortality of cancer. Currently some 13 million new cancers are diagnosed annually
and cancer is estimated to be the 2nd to 3rd leading cause of death. How advanced the cancer is at time of diagnosis, together with the origin and type of cancer are important determinants
for the outcome and choice of best treatment regime for a cancer patient.
Figure 2. Examples showing the appearance of breast cancers in radiology (mammography), excised tumor specimen, and pathology (microscopy).
Cancer - clinical aspects
The symptoms for cancer are highly variable and depend on extent and localization of tumor growth. Clinical examination, radiologic investigations and laboratory tests can give clues to a cancer diagnosis, however, the firm diagnosis of cancer is ascertained by microscopical evaluation of tumor tissue. The information retrieved from microscopical examination defines the cancer diagnose and forms the basis for classification of the tumor type that allows for estimations of prognosis and prediction of best treatment regime.
Pathology
Several systems for classification of cancer exist. Firstly, cancer is classified based on the site of origin and tumor type with respect to differentiation and morphological features.
Most common are epithelial tumors, mainly adenocarcinoma followed by squamous cell carcinoma. Non-epithelial tumors include sarcomas (derived from mesenchymal cells),
lymphoma and leukemia (derived from hematopoietic and lymphoid cells), melanoma
(derived from melanocyte) and glioma (derived from glial cells). Cancer stage is important to predict the prognosis of a given cancer type.
Staging of cancer is performed using the TNM-classification system where the extent of tumor growth at the time of diagnosis is assessed for the primary tumor (T), eventual metastasis in
lymph nodes (N) and eventual metastasis in distant organs (M). Independent of tumor stage, the malignancy grade provides prognostic information and different cancer grading systems have been defined.
Examples of such include Gleason grading of prostate cancer and Elston-Ellis grading of
breast cancer. These systems estimate the degree of differentiation, proliferation and cellular atypia in a cancer based on
the microscopical appearance. For several forms of cancer, entities that reflect the stage of development from precursor states to invasive cancer have been defined and can be diagnosed
by microscopical examination. Examples include low grade adenoma-to-high grade adenoma-to colon colon cancer,
dysplastic melanocytic nevus-to-melanoma in situ-to-invasive melanoma, prostate intraepithelial neoplasia (PIN)-to-invasive prostate cancer
and ductal breast cancer in situ (DCIS)-to-invasive ductal breast cancer. In addition to microscopical examination,
molecular tests such as the analysis of gene mutations, gene expression and protein expression can add important diagnostic, prognostic and treatment predictive information.
Figure 3. Examples of HE-stained tissue sections representing the most common forms of human cancer.
Oncology
The choice of treatment for patients with cancer depends on the tumor type, malignancy grade and tumor stage at the time of diagnosis. Surgery with the ambition to remove the tumor is often the first choice of treatment when possible. Radiation and cytotoxic agents (chemotherapy) form the basis for treatment of tumors not eligible for surgery, such as leukemia and lymphoma, and can also be used to supplement surgery in patients at high risk for recurrence (adjuvant therapy) or replace surgery in cases where surgery is no longer a possibility due to the extent of tumor growth. Chemotherapy and radiation used for adjuvant treatment, aims to eradicate non-detected residual tumor cells after surgery to improve the chance of cure or prolong survival of the patient.
Tumor biology
Cancer is a cellular disease that originates from one malignantly transformed normal human cell. Although cancer is common in humans, cancer is a rare cellular event with a risk of 1/10000 billion (1/1016) for a normal cell to become a cancer cell. Cancer is a genetic disease caused by mutations of genes that transform the normal growth control and behaviour of cells to abnormal cancer cells that lack growth control. Cancer is believed to develop through a multi-step process, originating from the malignant transformation of one cell leading to subsequent steps of growth advantage compared to normal cells. The impaired growth control allows for the selection of cell clones with the highest rate of cell division and survival. Eventually the primary tumor acquires the ability to grow invasively into normal surrounding tissue followed by spread of cancer cells through the lymphatics and/or blood system to draining lymph nodes and distant other organs.
In addition to cancer cells themselves, solid forms of cancer also consists of surrounding cancer stroma that supports the tumor growth. The cancer stroma includes an extracellular component (matrix proteins) and various populations of normal cells such as fibroblasts, vascular cells and inflammatory cells. The host response evoked by tumor cells includes the development of stroma but also other forms of immunologic response. Signals from normal cells in the cancer stroma, including inflammatory cells can either support or inhibit growth of cancer cells.
Certain traits define cancer cells and distinguish the difference between cancer cells and normal cells. Despite the heterogeneity of cancer, general characteristic hallmarks of cancer have been identified (Figure 4) and underlying cellular signaling pathways that are dysregulated in cancer have in part been elucidated (Figure 5).
Figure 4. Schematic displaying characteristic hallmarks of cancer. Image from Hanahan & Weinberg, 2011. Elsevier user licence.
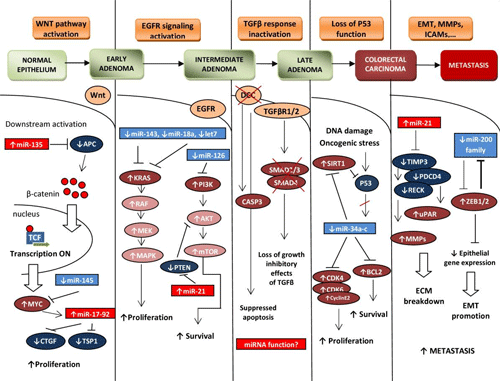
Figure 5. Example of signaling pathways involved in colon cancer. Image from Slaby et al., 2009. Creative Commons licence.
Relevant links
Uhlen M et al, 2017. A pathology atlas of the human cancer transcriptome. Science.
PubMed: 28818916 DOI: 10.1126/science.aan2507
Uhlén M et al, 2015. Tissue-based map of the human proteome. Science
PubMed: 25613900 DOI: 10.1126/science.1260419 Lawrence MS et al, 2014. Discovery and saturation analysis of cancer genes across 21 tumour types. Nature.
PubMed: 24390350 DOI: 10.1038/nature12912 Tamborero D et al, 2013. Comprehensive identification of mutational cancer driver genes across 12 tumor types. Sci Rep.
PubMed: 24084849 DOI: 10.1038/srep02650 Catalogue of somatic mutations in cancer - COSMIC (Sanger Institute)
Genes, Cancer, and DNA mutations - Tumor Portal (Broad Institute)
Cancer genome data from TCGA - The Cancer Genome Atlas (NIH)
Incidence, mortality, and prevalence of cancer - Cancer Today (IARC/WHO)
Microscopical images of cancer - Cancer Dictionary (Human Protein Atlas)
|
 The Human Protein Atlas project is funded
The Human Protein Atlas project is funded



 MENU
MENU